When a Payer Concern Becomes a Provider Problem Too
When Medicare Advantage payments made to insurers fail to keep pace with rising medical costs, insurers have limited levers.
They can’t renegotiate what CMS pays them. What they can do is become more aggressive downstream—but changing how, when, and under what conditions they pay providers.
And that’s when providers start to feel the pressure—not in rate sheets, but in claim denials, silent underpayments, and slower cash.
From an RCM standpoint, this is a familiar cycle. What’s different now is how expensive and risky it’s become to manage this pressure with traditional AR workflows.
Historically, with insurers have responded to Medicare Advantage policy shifts by:
None of these have ever been labeled as “rate cuts.” But the net impact on providers remained the same: slower, less predictable cash.
Prior Authorization: Another Revenue Risk Leaders Can’t Ignore
Payment pressure isn’t the only force at play. According to Kaiser Family Foundation, Medicare Advantage insurers made nearly 53 million prior authorization determinations in 2024 alone—a clear sign of how aggressively payers are managing utilization and reimbursement.
For providers, this translates into:
Interestingly, more than 80% of denied prior authorization requests that were appealed in 2024 were subsequently overturned, underscoring how critical strong appeal workflows and claim prioritization in AR management play in today’s reimbursement landscape.
How Jindal Healthcare’s Revenue Cycle AI Mitigates These Risks
Jindal Healthcare’s revenue intelligence platform is built specifically for high-volume, high-friction, high-scrutiny reimbursement environments like Medicare Advantage.
It operates across three layers of AR workflows, supporting RCM teams through:
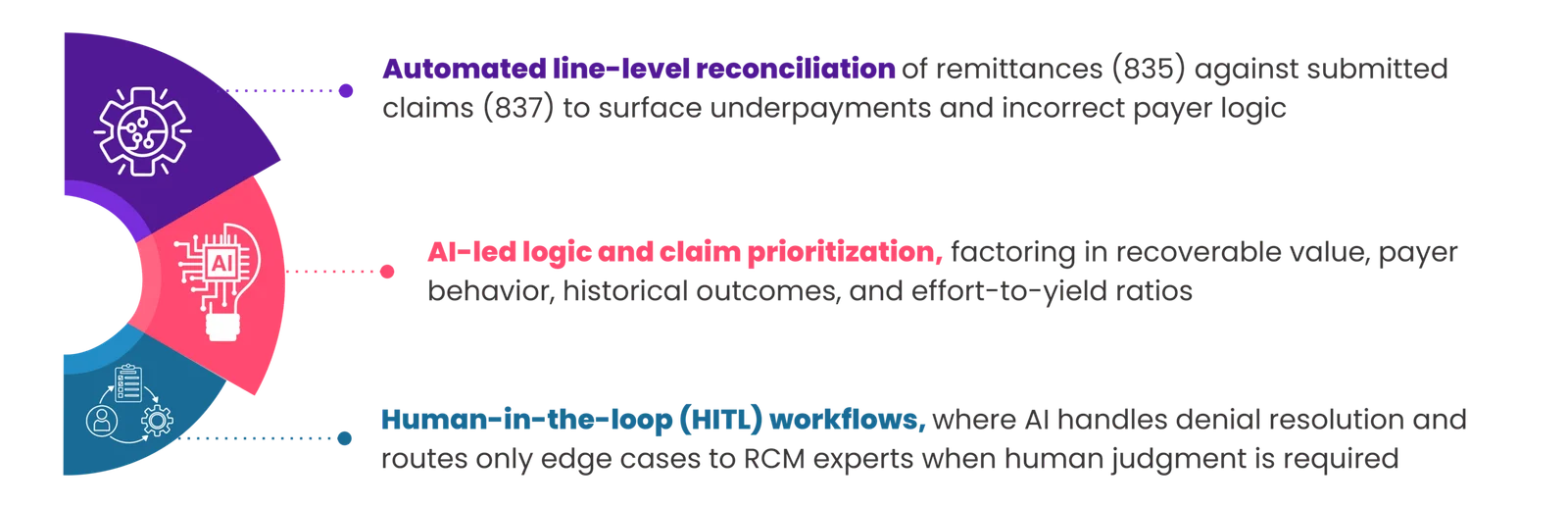
In parallel, it continuously analyzes denial and payment behavior by payer, CPT, modality, and ordering patterns—feeding insights back into front-end and mid-cycle workflows for proactive denial prevention.
The result is not just faster revenue recovery at a lower cost but fewer RCM issues cascading downstream later due to its continuous learning loop.
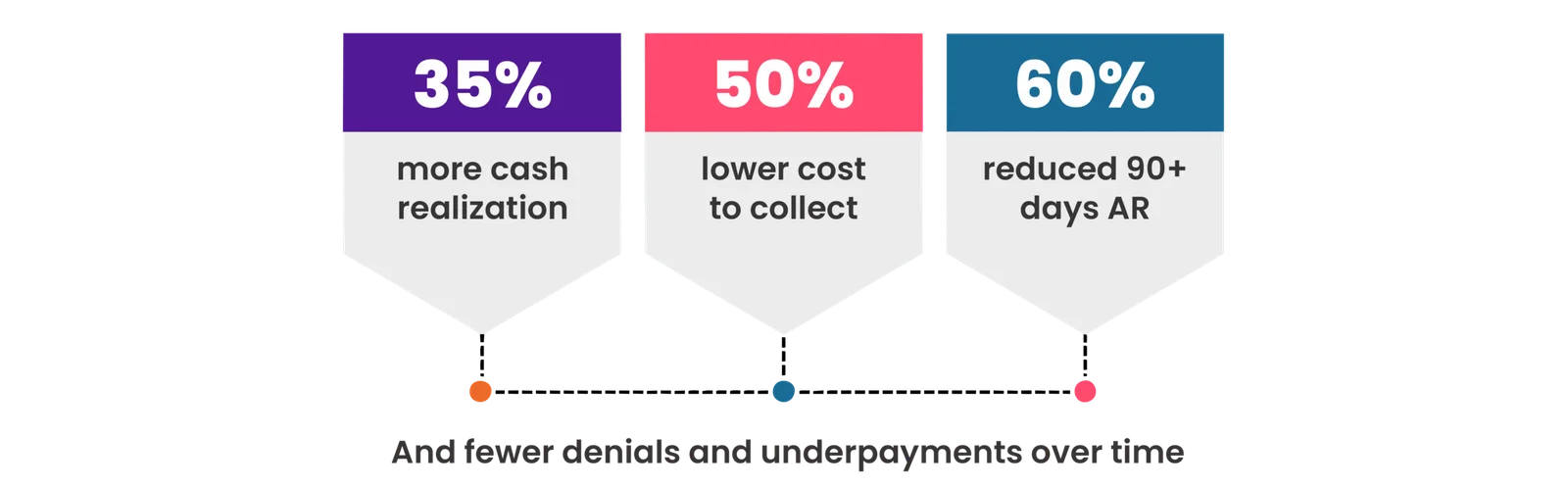
Organizations leveraging revenue intelligence-led RCM workflows report:
The Path Forward for Healthcare CFOs and RCM Leaders
For healthcare providers, the proposed Medicare Advantage payment outlook is clearly suggestive of continued margin pressure, more aggressive claim scrutiny, and greater volatility in cash flow. They must, therefore, leverage revenue intelligence to: